The bone structure of the knee joint is formed by the femur, the tibia, and the patella. The ACL is one of the four main ligaments within the knee that connect the femur to the tibia.
It is estimated that 70 percent of ACL injuries occur through non-contact mechanisms while 30 percent result from direct contact with another player or object.
The mechanism of injury is often associated with deceleration coupled with cutting, pivoting or sidestepping maneuvers, awkward landings or “out of control” play.
Immediately after the injury, patients usually experience pain and swelling and the knee feels unstable. Within a few hours after a new ACL injury, patients often have a large amount of knee swelling, a loss of full range of motion, pain or tenderness along the joint line and discomfort while walking.
Surgical Treatment
ACL tears are not usually repaired using suture to sew it back together, because repaired ACLs have generally been shown to fail over time.Therefore, a substitute graft made of tendon generally replaces the torn ACL. The grafts commonly used to replace the ACL include:
- Hamstring tendon autograft (autograft comes from the patient)
- Quadriceps tendon autograft
- Allograft (taken from a cadaver) patellar tendon, Achilles tendon, semitendinosus, gracilis, or posterior tibialis tendon
The goal of the ACL reconstruction surgery is to prevent instability and restore the function of the torn ligament, creating a stable knee. This allows the patient to return to sports. There are certain factors that the patient must consider when deciding for or against ACL surgery.
Patient Considerations
Active adult patients involved in sports or jobs that require pivoting, turning or hard-cutting as well as heavy manual work are encouraged to consider surgical treatment. This includes older patients who have previously been excluded from consideration for ACL surgery. Activity, not age, should determine if surgical intervention should be considered.
A patient with a torn ACL and significant functional instability has a high risk of developing secondary knee damage and should therefore consider ACL reconstruction.
It is common to see ACL injuries combined with damage to the menisci (50 percent), articular cartilage (30 percent), collateral ligaments (30 percent), joint capsule, or a combination of the above. The “unhappy triad,” frequently seen in football players and skiers, consists of injuries to the ACL, the MCL, and the medial meniscus.
As many as 50 percent of meniscus tears may be repairable and may heal better if the repair is done in combination with the ACL reconstruction.
Common Treatment Options
________________________________________________________________________________
Meniscus Removal or Repair
 The Orthopedic Surgeon may remove or repair damaged meniscal tissue. Torn tissue on the inside of the meniscus is often removed. Newly torn tissue on the outer edge of the meniscus can often be repaired. This tissue gets enough blood to heal properly.
The Orthopedic Surgeon may remove or repair damaged meniscal tissue. Torn tissue on the inside of the meniscus is often removed. Newly torn tissue on the outer edge of the meniscus can often be repaired. This tissue gets enough blood to heal properly.
________________________________________________________________________________
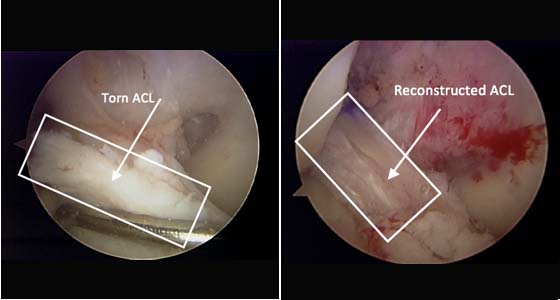
Ligament Reconstruction
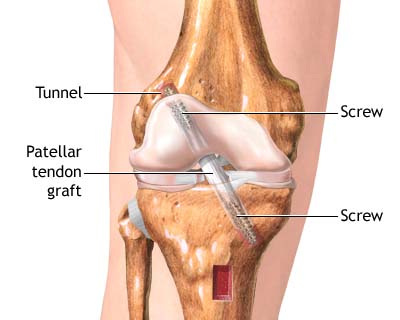 The Orthopedic Surgeon can reconstruct a damaged anterior cruciate ligament. The damage tissue is replaced with healthy, strong tissue (a graft). The graft may come from the patellar ligament or from another source.
The Orthopedic Surgeon can reconstruct a damaged anterior cruciate ligament. The damage tissue is replaced with healthy, strong tissue (a graft). The graft may come from the patellar ligament or from another source.
________________________________________________________________________________
Cartilage Shaving or Removal

 The Orthopedic Surgeon may smooth or shrink rough cartilage by shaving it or using a thermal device. Or, he may drill exposed bone to make the cartilage grow. Any loose bodies may be removed.
The Orthopedic Surgeon may smooth or shrink rough cartilage by shaving it or using a thermal device. Or, he may drill exposed bone to make the cartilage grow. Any loose bodies may be removed.
________________________________________________________________________________
Patella Smoothing or Release

 The Orthopedic Surgeon may smooth or shrink bands of cartilage under the patella by shaving them or using a thermal device. If the patella is tilted, he may clip bands of tissue. This is called a lateral release. It aligns the patella with the femur.
The Orthopedic Surgeon may smooth or shrink bands of cartilage under the patella by shaving them or using a thermal device. If the patella is tilted, he may clip bands of tissue. This is called a lateral release. It aligns the patella with the femur.
Please feel free to contact us with any questions. You may also always call us TOLL FREE: 866.509.0571 or +1817.405.2778 or SEND US AN EMAIL to info@orthopv.com